
By Joyclyn Wea, health reporter and New Narratives editors
Summary:
- Liberia’s new health deal with the United States is being presented as a major step forward giving the country the funds it needs to build a strong system.
- But experts warn it may actually bring less money, weaker oversight, and serious risks for corruption and public health.
- They warn that cuts to funding, threats to women’s health services, and broad access to Liberians’ medical data could leave the country more vulnerable, not stronger.
Late last year, the government of Liberia signed a five-year health agreement with the United States. President Joseph Boakai’s administration celebrated the deal as a step toward taking control of the country’s own health system. But health experts, former U.S. government officials, and civil society groups are raising serious concerns about what the agreement actually delivers — and what it leaves out.
The deal, known as a Health Compact, is part of the Trump administration’s new “America First Global Health Strategy.” Instead of funding health programs through international agencies and non-governmental organizations — the model the U.S. has used for decades — the new approach gives money directly to national governments. In Liberia’s case, that means up to $124 million paid out over five years, with the Liberian government responsible for spending it.
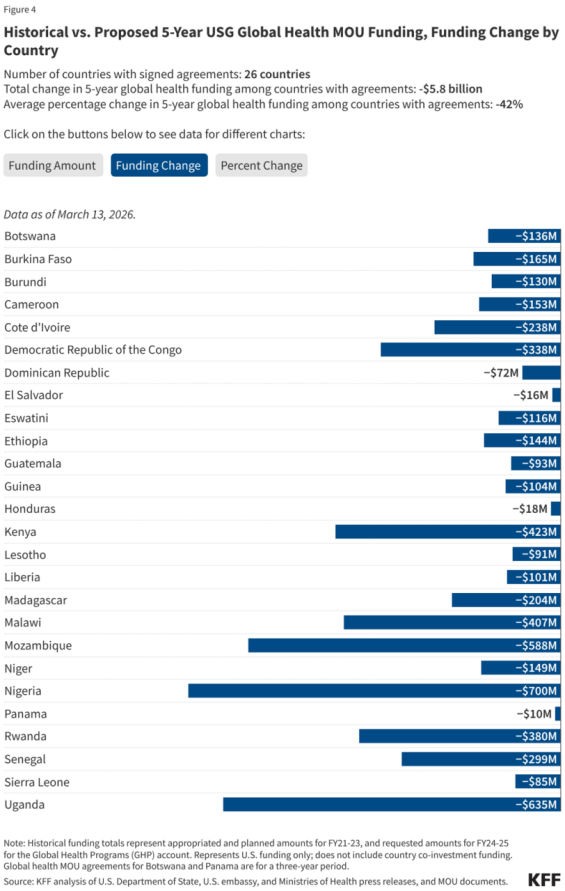
Liberia was the third country to sign, after Kenya and Rwanda. By mid-March 2026, the U.S. had struck similar deals with 26 African countries, representing nearly $20 billion in U.S. government commitments.
Supporters of the new model argue it gives African governments more control over their own health systems. But a range of experts in the field, including two former U.S. Agency for International Development (USAID) staff who worked in West Africa, have raised serious concerns about multiple aspects of the agreement.
A Fraction of What Came Before
To understand what is changing, it helps to know what is being replaced. Until earlier this year, the U.S. funded health programs in Liberia at roughly $70 million per year through USAID. That money supported everything from HIV and malaria treatment to maternal health clinics, community health workers, and disease surveillance systems.
When the Trump administration shut down USAID in early 2025, most of that funding stopped immediately. The new Health Compact offers around $25 million per year — a 63 percent reduction in annual U.S. health support compared to 2024 levels, according to the Center for Global Development.
The cuts are not evenly spread. One former USAID health officer who worked in West Africa until 2025 said the reduction in global health security funding — programs designed to detect and respond to outbreaks like Ebola — is particularly alarming. Liberia’s previous annual budget for that work was around $8 to $9 million. Under the new agreement, that figure drops to roughly $2.5 million.
“Who is going to detect something in seven days and mount a response?” the former USAID official asked. “The government was only able to do that because of the partners USAID was funding.”
The official, who has deep experience across West Africa, spoke on condition of anonymity for fear of retaliation from the Trump administration.

The Oversight Question
The previous U.S. government-to-government health program in Liberia — which ran from around 2011 and covered eight counties by the time it was discontinued — operated under a reimbursement model. The Liberian government could only receive funds after proving it had met specific health targets, verified by an independent third party at a cost of roughly one to two million dollars per year.
That system was not without problems. A high-profile corruption scandal in Margibi County — where funds meant for health services were misused — drew intense scrutiny. A 2024 State Department review also found that Liberia failed to meet eligibility criteria related to addressing corruption, which placed the entire program under review before USAID was shut down.
The new Health Compact does not include a comparable verification mechanism. The former USAID official said she has been unable to get a clear answer on how funds will be tracked. “I don’t think they care about the oversight,” she said. “I think they’re just going to give them the money and ask for some good results they can share.” A second former official with West Africa experience warned that removing oversight infrastructure could make corruption worse, not better — since even the old system’s imperfect accountability had provided some check on how money was spent.
The Informal Working Group on Reproductive Rights and Health in Liberia, a coalition of local and international organizations, raised similar concerns in a February 2026 letter to Health Minister Dr. Louise Mapleh Kpoto. The MOU explicitly gives the U.S. the right to pause or terminate any programs that do not align with the current administration’s interests — a unilateral exit clause that critics say leaves Liberia with little protection if political winds in Washington shift.
The group also flagged a “funding cliff”: U.S. support for health commodities is scheduled to fall from over $10.5 million in 2026 to roughly $540,000 by 2030, with Liberia expected to cover the difference. The group warned this could cause serious shortages of essential supplies, including contraceptives and maternal health medicines.
Reproductive Health Left Out
The Health Compact focuses its disease surveillance funding on a narrow list: HIV/AIDS, tuberculosis, malaria, polio, and measles. The Working Group warned that this “siloed” approach leaves reproductive and maternal health services without dedicated support.
Aminata Kamara-Sneh, a reproductive health expert with the RFSU (Swedish Association for Sexuality Education), a non-profit organization promoting sexual and reproductive health and rights, says one of the most alarming aspects of the compact is how U.S. abortion restrictions will operate across the entire public health supply chain. The Helms Amendment — U.S. law since 1973 — bans American foreign assistance from being used for abortion services. The “Mexico City Policy,” known by its critics as the “Global Gag Rule,” goes further, barring recipient organizations from providing abortion referrals or advocating for abortion access even with their own money. Under Trump’s second term, the Gag Rule has been expanded to apply not just to NGOs but to governments with U.S. aid agreements — meaning the restrictions could bind the Liberian government across its central medical warehouse and commodity supply chain serving all counties.

Sneh points to the first Trump administration, where contraceptive supplies from central warehouses in the counties covered by U.S. funding were removed — and expects the same will happen again. The stakes are high for Liberians. Already, 628 women die out of every 100,000 who give birth, according to the World Health Organization. A 2021 study found nearly 38,000 women seek abortion each year – but, because abortion is mostly illegal and done by secretive, dangerous methods, more than three in every five led to moderate to severe complications, and one in ten resulted in death or “near misses”.
“If post-abortion care is not available, then our maternal mortality rate, which is already one of the highest across the region, could increase,” according to reproductive health specialist Aminata Kamara-Sneh.
“If women and girls cannot have access to the commodities that they need to prevent unwanted pregnancy, then I want to see if the abortion rate will also increase,” said Dr. Su Mon Thaw, DKT’s country manager.

The Working Group flagged another problem buried in the agreement’s data. The WHO lists Liberia’s maternal mortality rate to be 628 deaths per 100,000 live births, according to estimates. But the agreement uses a baseline of just 116 per 100,000 — a figure far below the national reality. Because the U.S. reserves the right to cut funding if benchmarks are not met, the group warned that this creates a trap: Liberia could lose support for failing to achieve gains that were never statistically realistic.
Experts Flag Release of Liberians’ Sensitive Data
Beyond the headline funding figures, experts have raised alarms about conditions embedded in the agreement. The MOU requires Liberia to provide the U.S. with extensive, real-time access to national health data systems — including electronic medical records, disease surveillance platforms, and laboratory information systems — in some cases for up to 25 years. Liberia currently has no comprehensive national data protection law. The Working Group warned that this level of external access may conflict with Article 16 of Liberia’s constitution, which protects the right to privacy.
Virology professor Oyewale Tomori, a former WHO regional virologist who has reviewed the Africa-wide compact agreements, has raised broader concerns about the data provisions across all 26 deals. African countries, he argued in The Conversation, should not sign away health data or pathogen samples — which have significant commercial and scientific value — without guarantees of access to any resulting medical innovations. For every dollar invested in COVID-19 vaccine development, estimated returns ranged from $42 to $775. The potential returns from innovations derived from any of these pathogens, Tomori wrote, could far exceed the total U.S. contributions to the agreements. Zimbabwe has rejected the deal for this reason.
A Broader Bargain?
Liberia’s health deal did not happen in isolation. The Trump administration has been using health compacts, alongside the threat of aid cuts, tariffs, and visa restrictions, to secure a range of concessions from African governments. At least four countries that signed health deals had previously agreed to accept third-country deportees — people deported from the U.S. to countries they have no ties to. In Zambia, a health agreement has been explicitly linked to a cooperation deal in the mining sector. When Zambia resisted, the Trump administration considered withholding crucial HIV Aid, according to a draft memo seen by the New York Times.
Liberia has acquiesced to at least one Trump demand. In October the Department of Homeland Security announced that Liberia had agreed to accept third-country nationals deported from the U.S., confirmed in court filings involving a Salvadoran man with no connection to Liberia. The State Department has officially denied any link between health compacts and deportation or investment deals.
Professor Tomori argues that African governments moved too quickly and too individually. Had they mandated the African Union and Africa CDC to negotiate collectively, they would have been in a far stronger position. Instead, what emerged was a set of bilateral agreements designed, in his assessment, primarily for the benefit of the donor.
New Narratives sought comment from Dr. Louise Mapleh Kpoto, Liberia’s health minister, on the concerns raised about the deal, but she did not respond to emails.
What Happens Next
At a deeper level, the debate over the Health Compact reflects a long-running tension in global health: how much external funding helps, and how much it creates a dependency that makes health systems more fragile. Liberia is an extreme case. At its peak, the USAID health office in Liberia managed a budget roughly equivalent to the entire Ministry of Health’s annual government allocation — decades of investment that saved lives but also built a system that experts say could not survive without outside money and outside oversight.
The Liberian government has expressed optimism that the new model gives it more direct control, bypassing the large international implementing organizations through which as much as 75 percent of old USAID funding once flowed. But whether the government has the systems, accountability structures, and political will to spend the money well remains unanswered.
A February opinion piece by Africa CDC Director-General Jean Kaseya, AU Commission Chair Mahmoud Ali Youssouf, and former Ghanaian President John Mahama noted that up to 40 percent of Africa’s health spending is lost to inefficiency each year — and argued that the answer is stronger institutions, not swapping one form of dependency for another. Professor Tomori echoes that view, contending that the co-investment requirements in the compacts — which oblige African governments to progressively increase their own health spending — sound promising in theory but are almost certainly unrealistic in practice.
African countries collectively committed to allocating 15 percent of national budgets to health under the 2001 Abuja Declaration. Not one has consistently met that target in 25 years.
The Working Group has called on the Ministry of Health to publish the full compact, including financial and data-sharing annexes, for public and parliamentary review, and to include civil society in the 90-day implementation planning process. It has not yet received a response. With USAID effectively gone and the Global Fund also facing U.S. funding cuts, there are few places left to turn if things go wrong.
“I would not want to be the president of Liberia right now,” one former USAID official said, “trying to build the health system effectively with this money while keeping control of the corruption.”
This story was a collaboration with New Narratives as part of the Investigating Liberia project. Funding was provided by a private donor and the Swedish International Development Cooperation Agency. The donors had no say in the story’s content.